
PT-141 Research Guide: Melanocortin Receptor Signaling
Written bySpartan Research Team
Most pharmacological approaches to reproductive and sexual health research work at the tissue level. They target blood vessels, smooth muscle, or hormonal receptors in peripheral organs. PT-141 (bremelanotide) goes upstream. It targets melanocortin receptors MC3R and MC4R in the brain, initiating a CNS-driven signaling cascade. That’s the core distinction that made it an interesting research tool from the beginning and led to FDA approval of bremelanotide (Vyleesi) in 2019 for a condition that peripheral-acting agents hadn’t adequately addressed.
This guide covers the full PT-141 research story: the Palatin Technologies development history, the receptor-level mechanisms, how MC3R and MC4R differ and where they’re expressed, how central signaling compares to peripheral pharmacological approaches, and what the clinical trial record shows. It’s a compound with a genuinely unusual mechanism and a richer research history than most researchers realize.
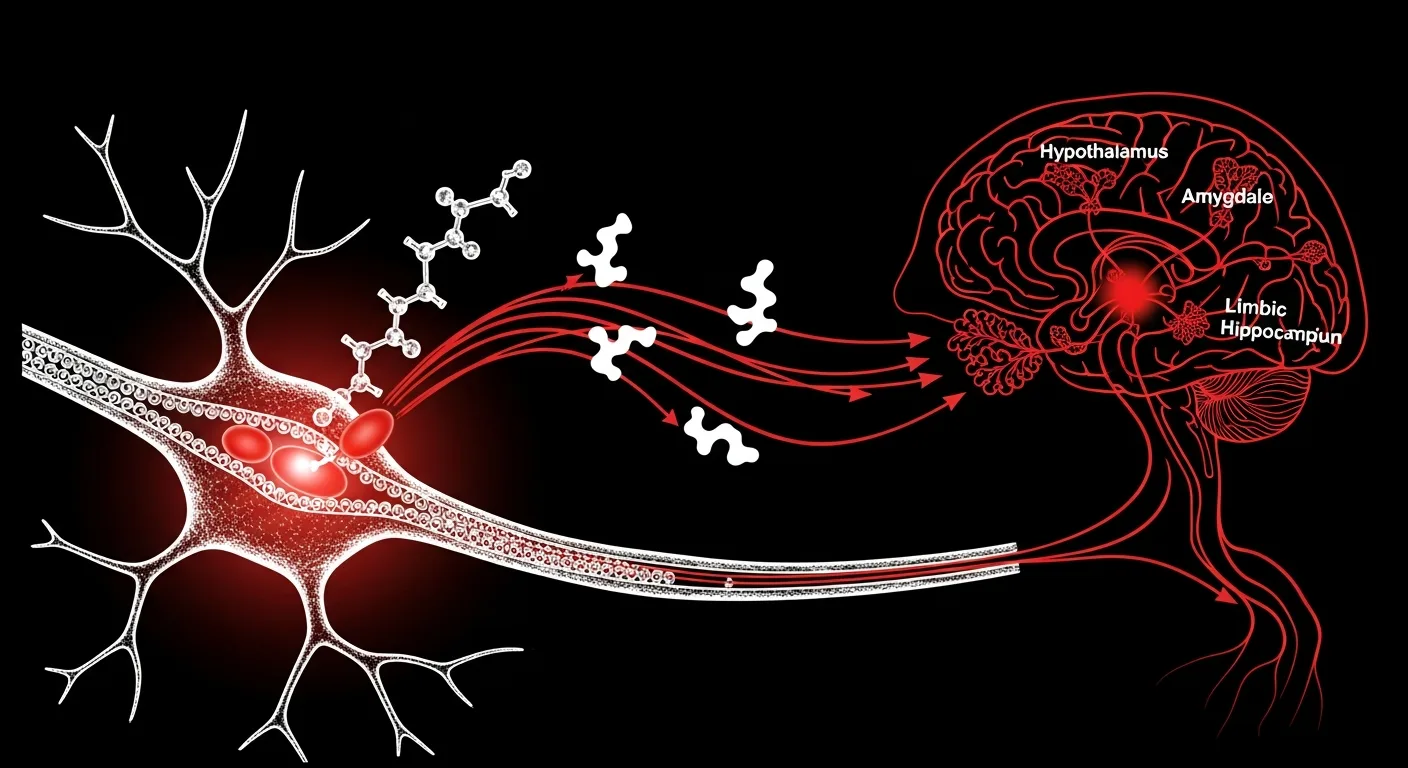
- PT-141 binds MC3R and MC4R in the CNS, with MC4R in the paraventricular nucleus of the hypothalamus considered the primary site for pro-sexual signaling effects
- Mechanism is centrally mediated (CNS), distinct from peripherally-acting PDE5 inhibitor approaches
- Palatin Technologies developed PT-141 from MT-II (melanotan II), modifying it to reduce tanning side effects while preserving central activity
- Molinoff et al. (2003) published foundational Phase 1 pharmacokinetic and safety data
- Pfaus et al. (2010) conducted extensive preclinical behavioral research establishing the MC4R pathway for pro-sexual signaling
- FDA approved bremelanotide as Vyleesi in 2019 for hypoactive sexual desire disorder in premenopausal women

The Melanocortin System: Background and Receptor Biology
The melanocortin system is one of those biological networks that turns out to be involved in far more than its name suggests. “Melanocortin” comes from the original discovery of melanocyte-stimulating hormones (MSH peptides), which control skin pigmentation. But the system’s reach extends to energy balance, stress response, inflammation, cardiovascular regulation, immune function, and yes, reproductive behavior.
Five melanocortin receptors exist (MC1R through MC5R), each with distinct tissue distribution and function. MC1R on melanocytes controls pigmentation. MC2R on adrenal cells responds to ACTH. MC3R and MC4R are the CNS-predominant receptors with roles in energy homeostasis and behavioral regulation. MC5R is found in exocrine glands. PT-141 selectively engages MC3R and MC4R among these five subtypes.
All melanocortin receptors are GPCRs coupled to Gs proteins. Activation increases intracellular cAMP via adenylyl cyclase, which activates PKA and downstream gene expression changes. But the specific downstream effects depend entirely on the cell type expressing the receptor and the neural circuits that cell participates in. MC4R in the paraventricular nucleus (PVN) of the hypothalamus sits at the intersection of multiple behavioral and autonomic regulatory pathways, which is why it’s such an interesting research target for reproductive behavior studies.
Development History: From Melanotan to Bremelanotide
PT-141’s story starts with an accident of sorts. Researchers at the University of Arizona were investigating MT-II (melanotan II), a potent non-selective melanocortin agonist originally developed as a tanning agent. MT-II worked for tanning, but human subjects in early trials reported an unexpected side effect: spontaneous sexual arousal. This was a CNS effect, not a peripheral vascular effect, and it was reproducible enough to be worth investigating seriously.
Palatin Technologies licensed the melanocortin-based compound program and set about designing a modified molecule that retained the CNS pro-sexual activity but reduced the tanning side effect (which was mediated by MC1R on melanocytes). The result was PT-141, also called bremelanotide: a cyclic heptapeptide derived from MT-II with modifications to reduce MC1R activity while preserving MC3R and MC4R affinity.
Molinoff et al. (2003, PMID: 14568756) published the first Phase 1 human pharmacokinetic data for PT-141. The compound showed good bioavailability by subcutaneous administration, a half-life of approximately 2.7 hours, and dose-dependent increases in subjective sexual desire measures in both male and female subjects. This was the foundational paper that established PT-141 as a viable development candidate.
Diamond et al. (2004, PMID: 15033442) followed with Phase 2 data specifically in male subjects with erectile dysfunction who had been inadequate responders to PDE5 inhibitors. The results were notable: PT-141 produced responses in men who didn’t respond to peripheral-acting agents, suggesting the CNS pathway it targeted was genuinely distinct and could be effective when the peripheral vascular mechanism was compromised.

MC3R and MC4R: Receptor Distribution and Functional Differences
Understanding PT-141’s mechanism requires understanding how MC3R and MC4R differ, both in where they’re expressed and what they do when activated.
MC4R has the broader CNS distribution of the two. It’s expressed throughout the hypothalamus (especially the PVN, ARC, and dorsomedial nucleus), in limbic structures including the amygdala and hippocampus, in the brainstem, and in the spinal cord. This distribution pattern puts MC4R at nodes in circuits governing appetite, stress response, autonomic function, and behavior. MC4R knockout mice develop obesity (because of its role in energy homeostasis) and show altered behavioral responses including changes in proceptive behavior in female models.
MC3R has a narrower hypothalamic distribution and a role in energy balance regulation (particularly feedback regulation of MC4R activity via AgRP neurons). In the context of PT-141’s behavioral effects, MC4R is considered the primary effector receptor. Pfaus et al. (2010, PMID: 20045492) used selective receptor knockout and antagonist studies to demonstrate that MC4R in the medial preoptic area and PVN was required for melanocortin agonist-induced increases in proceptive behavior in female rats. MC3R antagonism had a smaller effect on these endpoints.
That said, MC3R shouldn’t be dismissed entirely. Its expression in limbic regions and its role in stress-responsive neural circuits suggests it contributes to the broader behavioral context. And PT-141’s dual MC3R/MC4R activity may produce effects that neither receptor mediates alone.
Central vs Peripheral: Why the Mechanism Distinction Matters
The mechanistic distinction between PT-141 and peripheral-acting pharmacological approaches is more than academic. It determines which research models are appropriate, which populations of subjects show responses, and what the approach can and can’t do.
Peripheral vascular approaches require an intact neurovascular reflex chain from CNS arousal signals down to peripheral tissue response. If any link in that chain is compromised (neurological, vascular, hormonal), peripheral agents have limited efficacy because they act at the end of the chain, not the beginning. PT-141 acts at the top of the chain, in the CNS. If the CNS circuitry is intact and the issue is downstream, PT-141 reaches the problem from a different direction.
This is exactly what Diamond et al. (2004) showed: responses in male subjects who didn’t respond to PDE5 inhibitors. It wasn’t that PT-141 was more potent at the vascular level; it worked through a different pathway entirely. And in research models designed to study desire or motivation rather than strictly peripheral physiological responses, the central mechanism is precisely the one of interest.
The central mechanism also explains PT-141’s observed behavioral profile in preclinical models. Pfaus’s group showed increases in proceptive behavior (active solicitation behaviors in female rodent models, not simply reflexive responses), a qualitatively different outcome from what peripheral vascular agents produce. This distinction is important for researchers designing studies around motivation, desire, or behavioral endpoints versus strictly physiological endpoints.
Clinical Trial Data and FDA Approval
Clayton et al. (2016, PMID: 27401904) published Phase 3 efficacy data that formed the basis of the eventual FDA submission. The trials focused on premenopausal women with hypoactive sexual desire disorder (HSDD), using validated instruments including the Female Sexual Function Index (FSFI) and a daily diary measure of satisfying sexual events. At the doses studied, bremelanotide produced statistically significant improvements on both endpoints versus placebo.
Nausea was the primary dose-limiting observation in Phase 3, occurring in approximately 40% of subjects at the approved dose. Flushing and transient blood pressure changes were also documented. The FDA approved bremelanotide as Vyleesi in 2019, making it the second approved drug for HSDD in women (after flibanserin/Addyi, a different mechanism involving serotonin and dopamine receptors).
The approval specifically covers premenopausal women with acquired, generalized HSDD. Researchers investigating PT-141 in other reproductive biology contexts, or studying the underlying melanocortin mechanism in behavioral models, work with PT-141 as a research compound. Our PT-141 product page provides information for qualified researchers. For related reproductive signaling research, our sexual health research peptides page and the companion article on kisspeptin vs enclomiphene mechanisms provide additional context on CNS reproductive signaling pathways.
Comparing Melanocortin Agonism to Other CNS-Targeting Approaches
PT-141 isn’t the only CNS-targeting research approach in reproductive behavior pharmacology. Flibanserin (Addyi) targets 5-HT1A and 5-HT2A serotonin receptors as well as dopamine D4 receptors, modulating the balance of excitatory and inhibitory neurotransmission in sexual motivation circuits. Kisspeptin acts on GnRH neurons to modulate the HPG axis upstream. These represent distinct points in a complex neural regulatory system.
What distinguishes PT-141 mechanistically is the specificity of the melanocortin system for behavioral activation (versus primarily hormonal regulation in the case of kisspeptin, or neurotransmitter rebalancing in the case of flibanserin). MC4R activation in the PVN produces direct behavioral outputs through descending spinal pathways and autonomic projections. It’s a more direct “brain to body” pathway for behavioral responses than HPG axis modulation, which operates on a longer timescale through hormonal intermediaries.
For researchers designing protocols to distinguish these mechanisms, PT-141’s well-characterized receptor pharmacology and the availability of selective MC3R and MC4R antagonists makes it a useful research tool for dissecting melanocortin contributions from other signaling pathways.
PubMed Citations
- Molinoff PB et al. (2003). “PT-141: A melanocortin agonist for the treatment of sexual dysfunction.” Ann N Y Acad Sci. PMID: 14568756
- Diamond LE et al. (2004). “Effect of PT-141, a melanocortin receptor agonist, on erection in men with erectile dysfunction.” J Sex Med. PMID: 15033442
- Pfaus JG et al. (2010). “The roles of melanocortins and their receptors in male and female sexual behavior.” Physiol Behav. PMID: 20045492
- Clayton AH et al. (2016). “Bremelanotide for female sexual dysfunctions in premenopausal women.” Obstet Gynecol. PMID: 27401904
Research Disclaimer: All products sold by Spartan Peptides are intended for laboratory and in vitro research purposes only. Not for human consumption. These statements have not been evaluated by the Food and Drug Administration. Products are not intended to diagnose, treat, cure, or prevent any disease. For research use only.
Written by the Spartan Research Team
Our team of peptide researchers and biochemists reviews every article for scientific accuracy. Learn more about our team →